가톨릭 신앙생활 Q&A 코너
|
우한 폐렴 실시간 감염자, 사망자 및 회복자들의 전세계적 그래픽 가시화 누계 분포 - 미국 존스 홉킨스 대학교 CSSE 제공 2029_ |
||||||
|---|---|---|---|---|---|---|
|
2020-02-02 ㅣ No.2029 게시자 주: 본글의 인터넷 주소, http://ch.catholic.or.kr/pundang/4/soh/2029.htm 에 접속하면, 본글 중에서 제시되고 있는 출처 문헌들을 쉽게 확인할 수 있습니다. 그리고 다음의 인터넷 주소, http://ch.catholic.or.kr/pundang/4/q&a.htm 에 접속하면, 본글의 제목이 포함된, "가톨릭 신앙생활 Q&A 코너" 제공의 모든 게시글들의 제목들의 목록을 가질 수 있습니다. 또한 (i) 2006년 12월 16일에 개시(開始)하여 제공 중인 미국 천주교 주교회의/중앙협의회 홈페이지 제공의 날마다 영어 매일미사 중의 독서들 듣고 보기, 그리고 (ii) 신뢰할 수 있는 가톨릭 라틴어/프랑스어/영어 문서들 등은, 다음의 주소들에 접속하면, 손쉽게 접근할 수 있습니다: http://ch.catholic.or.kr/pundang/4/ (PC용, 날마다 자동으로 듣고 봄) [주: 즐겨찾기에 추가하십시오]; http://ch.catholic.or.kr/pundang/4/m (스마트폰용) [주: 네이버 혹은 구글 검색창 위에 있는 인터넷 주소창에 이 주소 입력 후 꼭 북마크 하십시오]
+ 찬미 예수님!
[내용 추가 일자: 2020년 2월 20일, 18:30] 4-3. 이 전염병의 여러 특징들 중의 하나가 본인이 감염되었음을 전혀 알지 못하는 상태에서 상당한 기간[주: 약 2주]에 걸쳐 다른 이들을 감염시킬 수 있는 점인데, 다음의 주소에 접속하면, 국내의 상황을 실시간으로 확인할 수 있으며, 특히, 예를 들어, 감염자로 확진되지 않는 상태인 무증상 상태로 있으면서 그리하여 이 전염병의 최종 전파자로 머물러 있으면서, 장,노년들인 가족들에게 전파할 가능성이 높은 연령대가, 초,중,고 청소년들 및 대학생들이 포함되는, 20대 혹은 그 이하의 전 연령층들일 수 있음을 추정할 수 있는 통계 자료 "확진자 동선"를 접할 수 있습니다:
https://wuhanvirus.kr/ <------ 여기를 클릭하여 확인하십시오
[내용 추가 일자: 2020년 3월 16일] 출처: https://news.chosun.com/site/data/html_dir/2020/03/16/2020031600009.html [제목: 가장 힘들고 위험한 일 시켜달라… 이름 노출은 원치 않던 그 의사들] (발췌 시작) ―확진됐다가 완치된 환자에 의하면 고통이 가슴을 쥐어뜯듯이 그렇게 심하다고 하더군요. (이상, 발췌 끝) [이상, 2020년 3월 16일자 내용 추가 끝] [내용 추가 일자: 2020년 3월 18일] 다음의 주소에 접속하면, "신종 코로나바이러스 전염병 치료에 한약 청폐배독탕 이 도움이 된다고 합니다" 제목의 글을 읽을 수 있습니다: http://ch.catholic.or.kr/pundang/4/soh/2037.htm <----- 필독 권고 [이상, 2020년 3월 18일자 내용 추가 끝]
4-4. 그리고 인문학 전공자들, 응용 인문학 전공자들, 그리고 사회과학 전공자들도 읽고 충분히 잘 이해할 수 있도록 작성된, 아래의 제1-3항과 제2-3항에서 이미 지적한 바를 약간 더 자세하게 말씀드리면 다음과 같을 것입니다:
(i) 이번 전염병의 인(因, cause, 원인)은 신종 코로나바이르스 COVID-19이며, 그러나 이 인(因, cause, 원인)을 예방하는 백신과 치료할 치료제 둘 다는 아직 없음.
(ii) 이번 전염병의 연(緣, conditions, 조건)들은, 병원체들의 활동에 절대적으로 영향을 끼치는, (가) 양분(nourishment)인 사람의 몸(body), (나) 대기의 온도(temperature), 그리고 (다) 대기의 습도(humidity)임.
(iii) 이번 전염병의 연(緣, conditions, 조건)들 중에서, (나) 대기의 온도(temperature)와 (다) 대기의 습도(humidity)는, 자연 법칙에 따라 변화하므로, 사람이 인위적으로 통제할 수 없음.
(iv) 따라서, 이번 전염병의 연(緣, conditions, 조건)들 중에서, 양분(nourishment)인 사람의 몸(body)은, 감염자들과의 접촉을 미연에 차단함으로써, 사람이 인위적으로 이번 전염병의 창궐을 방지할 수 있는 유일한 수단임.
(v) 그러나 정치적 진영 논리에 빠져 있는, 외교적, 경제적 이해득실을 무엇보다도 우선적으로 따지는, 우리나라 정부 유관 부서 공무원들 및 방역 조치 결정권자들 중의 일부로 구성된 최종 결정권을 행사하는 기득권자들이 자신들이 추구하는 목적인(目的因, the final cause)인 세속적(secular) [명예, 돈, 권력, 혹은 특정 사상(思想)의 보급/구현 등에 대한] 과도한 욕망(inordinate desires)들을 판단의 잣대들/기준들로 여태까지처럼 계속 사용하기 위하여, 아직까지 위의 (i) - (iii)을 인정하지 않고 있음.
(vi) 그런 다음에, 아래의 제2-3항의 (iv)에서 말씀드린 바처럼 진행할 것 같음. [이상, 2020년 2월 20일, 18:30 내용 추가 끝]
[내용 추가 일자: 2020년 2월 15일, 12:00] 4. 4-1. 다음의 주소들에 접속하면, 아프리카에서 처음으로 창궐하였던 에볼라 바이르스용 항바이르스제로 개발된 Remdesivir이 메르스 감염의 예방 및 치료헤 효과가 있음이 히말라야 원숭이들에 대한 임상 실험에서 입증되었으며, 따라서, 작년 연말에 중국 후베이 성 우한 시에서 처음으로 창궐하기 시작한 신종 코로나바이러스(COVID-19) 감염의 예방 및 치료에 효과가 있을 수도 있기에, 이 약의 임상 실험이 [2020년 2월 6알자로] 중국 등에서 지금 진행 중이라는 2020년 2월 13일자 뉴스를 접할 수 있습니다:
출처 1: https://www.niaid.nih.gov/news-events/remdesivir-prevents-mers-coronavirus-disease-monkeys 출처 2: 'CORONAVIRUS" "NIAID" "Remdesivir" [구글 검색 결과] 출처 3: https://en.wikipedia.org/wiki/Remdesivir (출처 3으로부터 발췌 시작)
In response to the 2019–20 Wuhan coronavirus outbreak induced by coronavirus 2019-nCoV, Gilead provided remdesivir for a "small number of patients" in collaboration with Chinese medical authorities for studying its effects.[16] Gilead also started laboratory testing of remdesivir against 2019-nCoV. Gilead stated that remdesivir was "shown to be active" against SARS and MERS in animals.[17]
In late January 2020, remdesivir was administered to the first US patient to be confirmed to be infected by 2019-nCoV, in Snohomish County, Washington, for "compassionate use" after he progressed to pneumonia. While no broad conclusions were made based on the single treatment, the patient's condition improved dramatically the next day,[18] and he was eventually discharged.[19] Also in late January 2020, Chinese medical researchers stated to the media that in exploratory research considering a selection of 30 drug candidates, three of them, remdesivir, chloroquine and lopinavir/ritonavir, seemed to have "fairly good inhibitory effects" on 2019-nCoV at the cellular level. Requests to start clinical testing were submitted,[20][21] and on February 6, 2020 a clinical trial of remdesivir began in China.[22] (이상, 발췌 끝)
4-2. 그리고 다음의 주소에 접속하면, 위의 뉴스의 근거인 전문 학술지, Proceedings of the National Academy of Sciences에 실린 논문[제목: Prophylactic and therapeutic remdesivir (GS-5734) treatment in the rhesus macaque model of MERS-CoV infection] 전문을 읽을 수 있습니다: https://www.pnas.org/content/early/2020/02/12/1922083117 [이상, 2020년 2월 15일, 12:00 내용 추가 끝]
1. 1-1. 다음의 주소에 접속하면, 미국 존스 홉킨스 대학교 CSSE (The Johns Hopkins University, Center for Systems Science and Engineering) 제공의, 유관 나라별, 소위 말하는, 우한 폐렴 실시간 감염자, 사망자, 그리고 회복자들의 전세계적 그래픽 가시화 누계 분포를 확인할 수 있습니다 [주: 스마트폰의 경우에, 반시계 방향으로 90도 회전한 후에 화면을 보시기 바랍니다]:
출처: https://www.gisaid.org/epiflu-applications/global-cases-betacov/ (발췌 시작) (이상, 발췌 끝)
1-2. 바로 위의 화면을 들여다보면, 특히, 지난 2020년 1월 20일부터 오늘 이 시각(2020년 2월 2일 14:30)에 이르기까지, 전체 감염자 수(14,556명)에 비하여 회복자 수(340명)가 매우 낮은 것을 알 수 있는데, 바로 이 통계로부터, 만약에 이 집계가 사실이라면, 많이 부족한 죄인인, 해당 분야에 문외한인, 필자가 생각하더라도, 아마도 장기전(長期戰)을 예상하여야 하지 않나... 하는 우려를 하고 있습니다.
1-3. 특히, 스마트폰 혹은 Chrome 환경 아래에서 바로 위의 화면의 한가운데 하단 부분을 확대한 후에 Data Sources 란에 있는 파란색칠을 한 글자들을 클릭하면, 원출처들 제공의 시계열(時系列, time series) 상의 코아 자료들과 이들에 대한 분석 결과들을 또한 읽을 수 있는데, 우리나라 정부 유관 부서 혹은 학계 어느 곳에서 이들 원출처들 제공의 정보들을 국내의 의학계 및 의료진에게, 아무런 중간 가공 행위 없이, 제공하고 있는지에 대하여, 필자는 알지 못합니다.
[내용 추가 일자: 2020년 2월 4일 16:30] 예를 들어, 다음의 주소들에 접속하면, 위의 제1-1항의 근거 자료들들 왁인할 수 있는데, 의료계 종사자들과 특히 우리나라 정부 유관 부서 공무원들 및 방역 조치 결정권자들의 필독을 강력하게 권고드립니다:
[날짜별: 나라별: 확진자 수, 사망자 수, 회복자 수 누계] [나라별: 확진자 수, 회복자 수, 사망자 수 각 누계의 시계열 세 개]
[내용 추가 일자: 2020년 2월 13일] 위의 주소들로의 접속 과부하로 인하여, 2020년 2월 12일부터, 다음의 주소에서 위의 누계들의 근거 자료들을 제공하기 시작함: https://github.com/CSSEGISandDATA/2019-nCoV [이상, 2020년 2월 13일자 내용 추가 끝]
특히, 바로 위의 주소에 있는 세 개의 자료들 각각을 잘 들여다보면, (i) 우한이 포함된 후베이 성의 경우에는 과포화로 인한 통제 불능(out of control)의 상태이고, (ii) 중국의 다른 지역들에서도 확진자들이 계속 증가하는 추세이므로, 따라서, 거의 불가능한 현실이지만, 심지어, 설사 확실한 치료법이 조만간 확보된다고 하더라도, 이제는, 자칫 더 머뭇거리다가 국내가 과포화로 인한 통제 불능이라는 최악의 상태에 빠져드는 것을 적극적으로 회피하기 위하여, 중국과 우리나라 사이의 사람들의 이동을 철저하게 금지하여야 하는 단계, 혹은, 이에 준하는, 국내로 들어오는 모든 교통수단(여기에는 항공기, 배, 그리고 유람선 등이 포함됨)의 탑승(搭乘) 전후 둘 다에 엄격한 통제(統制)/검역(檢疫) 조치를 시의적절(時宜適切)하게 취하여야 하는 단계임을 알 수 있다는 생각입니다. 그리고, 당연한 이야기이지만, 이러한 조치가 더 늦어질수록 국내의 상황도, 지금과는 달리, 더 나빠질 것으로 생각됩니다.
형이하학적 현실에 대한 자연 법칙의 지배는 세속의(secular) 사람들 사이의 관계를 주된 대상으로 하는 윤리법의 지배보다 절대적 우위에 있기 때문에, 방역 조치 결정권자들이 속하는, 그 대다수가 자연 과학 분야를 전공하지 않은 자들로 구성된, 국내의 유관 특정 집단이 그 고유한 윤리/도덕(morality)(*1)의 범주에 속하는 자신들의 세속의(secular) 이해득실 관련 과도한 욕망(inordinate desire)을 포기함으로써,(*2) 최악의 상황의 발생을 적극적으로 회피한 이후에, 윤리적 처신에 있어, 마땅히, 자연 법칙이 지배하고 있는 형이하학적 현실이 수용할 수 있는 범위 내에서, 특정 집단의 사익(private interest)이 아니라, 국민 건강이라는 공익(public benefit/interest)을 위한, 최선, 차선, 차차선의 선택을 포함하는, 공동선(common good)의 순차적 실천을 위하여 힘써 노력하여야 할 것입니다.(*3)
----- (*1) 다음의 주소에 접속하면, "윤리/도덕"(morality)이라는 번역 용어의 윤리학적 정의(definition)를 읽을 수 있다: http://ch.catholic.or.kr/pundang/4/soh/1284.htm <----- 필독 권고
(*2) 게시자 주: 다음의 주소에 접속하면, "과도한 욕망"(inordinate desire)에서 사용되고 있는 "과도한"(inordinate)이라는 형용사의 윤리학적 정의(definition)를 읽을 수 있다: http://ch.catholic.or.kr/pundang/4/soh/1675.htm <----- 필독 권고
그리고 다음의 파란색칠을 한 굵은 글자들을 클릭하면, "과도한 욕망"(inordinate desire)이라는 표현이 어떠한 문맥 안에서 일관성있게 사용되고 있는지, 따라서 그 의미를 더 명확하게 이해할 수 있다: "inordinate desire" site:ch.catholic.or.kr/pundang <----- 또한 필독 권고
(*3) 게시자 주: 다음의 주소에 접속하면, 가톨릭 교회의 사회 교리에서 가르치는 "공동선"(common good)이라는 용어의 정의(definition) 등을 읽을 수 있다: http://ch.catholic.or.kr/pundang/4/soh/2029.htm <----- 필독 권고 ----- [이상, 2020년 2월 4일 16:30 내용 추가 끝]
[내용 추가 일자: 2020년 2월 10일] 1-4. 1-4-1. 위의 제1-1항에 안내해 드린 자료뿐만이 아니라, 다음의 Worldometer 홈페이지 제공의 자료도 그동안 필자가 들여다보고 있었는데, 또한 참고하시기 바랍니다.
본 게시글에 재 방문하는 분들이, 위의 제1-1항에서처럼, 최신 정보가 추가될 때마다 실시간으로 Update되는 자료들을 손쉽게 확인할 수 있는 인터넷 홈페이지 구동 방식으로, 추가적으로 안내해드리는 이유는, (i) 비록 영어이기는 하나, 획득된 자료들에 대한 수학적 분석 방법들에 대한 설명을 포함하여, 상황 설명들을 독자들이 읽고서 쉽게 이해할 수 있는 평이한 문장들로 제공하고 있고, (ii) 위의 제1-3항에서 이미 지적한 문제점, 그리고 (iii) 위의 제1-1항 제공의 자료의 Update에 있어, 예상 밖의, 시간 지연(time delay) 문제 때문입니다.
[내용 추가 일자: 2020년 2월 12일] 특히 중국 이외의 지역에서의 경과들에 대한 분석의 결과들을 2020년 2월 12일부터 제공하기 시작하였는데, [이상, 2020년 2월 12일자 내용 추가 끝] 국내의 의료계, 유관 학계, 공무원들, 정책 결정자들, 언론계 종사자들 뿐만이 아니라, 모두들 또한 참고하시기 바랍니다:
[내용 추가 일자: 2020년 3월 3일] PC에서 접속할 때에 아래의 문제점이 우리나라 시각으로 어제 발생하였음을 알게 되었는데, 다음은 이 문제점과 관련하여 Worldometer 측에서 트위터에 올린 공지문입니다. 아래의 문제가 해결될 때까지, 당분간 PC에서의 접속은, 다음의 주소에 접속하여 여기 저기를 찾아보십시오: http://www.worldometers.info/coronavirus/coronavirus-death-toll/
그리고 필자가 확인한 바에 의하면, 스마트폰에서 접속할 떄에는 아래의 접속 장애 문제가 없었습니다:
(발췌 시작)
(이상, 발췌 끝) [이상, 2020년 3월 3일자 내용 추가 끝]
출처: http://www.worldometers.info/coronavirus/coronavirus-cases/#case-tot-outchina (발췌 시작) (이상, 발췌 끝)
1-4-2. 그리고 또한 위의 제1-1항과 제1-4-1항에 안내해 드린 자료들뿐만이 아니라, 다음의 WHO (World Health Organization, 세계 보건 기구) 홈페이지 제공의 Situation Reports(상황 보고들)도 그동안 필자가 들여다보고 있었는데, 또한 참고하시기 바랍니다.
본 게시글에 재 방문하는 분들이, 위의 제1-1항에서처럼, 최신 정보가 추가될 때마다 실시간으로 Update되는 자료들을 손쉽게 확인할 수 있는 인터넷 홈페이지 구동 방식으로, 추가적으로 안내해드리는 이유는, 위의 제1-3항에서 이미 지적한 문제점 때문입니다. 국내의 의료계, 유관 학계, 공무원들, 정책 결정자들, 언론계 종사자들 뿐만이 아니라, 모두들 또한 참고하시기 바랍니다:
출처: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (발췌 시작) (이상, 발췌 끝) [이상, 2020년 2월 10일자 내용 추가 끝]
2. 2-1. 다음의 주소들에 접속하면, 연중 2월과 3월 동안 우한의 기온이 우리나라 서울보다 약 5-6도 더 높은 것을 알 수 있습니다. 그리고 상대 습도도 약 20% 더 높은 것을 알 수 있습니다. [주: 우한 지역의 상대 습도는 매달 75%로 거의 일정함. (내용 추가 일자: 2020년 3월 15일) 따라서, 예를 들어, 가습기(humidifier)를 사용하여 실내의 상대 습도를 60% 이상 유지함으로써, 이 신종 코로나바이러스에 감염됨을 예방할 수 없을 것임을 그리 어렵지 않게 추론할 수 있음(이상, 2020년 3월 15일자 내용 추가 끝)]:
[우한] https://ko.wikipedia.org/wiki/%EC%9A%B0%ED%95%9C%EC%8B%9C [서울] https://ko.wikipedia.org/wiki/%EC%84%9C%EC%9A%B8%ED%8A%B9%EB%B3%84%EC%8B%9C
2-2. 지금 우리나라의 기온이 우한의 요즈음의 기온에 도달하지 않았으나 그러나 조만간 도달할 것이므로, 향후 우한 지역의 기온 변화에 따른 우한 지역의 우한 폐렴의 추이/경과를 또한 잘 지켜볼 필요가 있다는 생각입니다.
[내용 추가 일자: 2020년 2월 8일 01:50] 2-3. 바로 위의 제2-2항에서 지적한 바를 관찰한 이후에, 그 인과 관계(cause and effect relationship)를 더 분명하게 알아차릴 수 있을 것이지만, (i) 몇 년 전에 우리나라에 창궐하였던 메르스와 지금 창궐 중인 우한 폐렴 둘 다가 유사한 코로나바이러스들에 의한 것임, (ii) 경제적 이유 때문에 엄격한 통제가 어려운 교통/관광 등의 현실적 여건 아래에서,(*4) 우한 폐렴의 원인인 신종 코로나바이러스의 지수 함수적(exponential) 전염력 [주: 현재까지 파악된 바에 의하면, 적어도 숫자 2의 n 승, at least 2 to the n; 주요 감염 경로: (i) 직접 전파(비말 전파 포함), (ii) 에어로졸 전파(공기 전파)(*5), (iii) 접촉 전파], (iii) 여태까지 과포화되어(oversaturated) 통제 불능(out of control)의 상태에 머물러 있는 중국 후베이성의 상황과 중국의 다수의 대도시들에서 지금까지도 확산 중인 상황, 그리고 특히, (iv) 몇 년 전에 우리나라에 창궐하였던 메르스가 우리나라에서, 무슨 특효약/치료제 때문이 아니라, 6월 말 경 우리나라에 고온다습한 장마전선이 형성된 이후에, 그리하여, "因緣(인연)" = "causes(因, hetu, 원인들) and conditions(緣, pratyaya, 조건들)"에 의한 변성(變成)함/성위(成為)함(becoming)에 있어 소위 말하는 한 개의 연(緣)(a condition)에 해당하는,(*6) 수많은 미생물들의 활동이 대단히 활발하게 된 이후에, 비로소 사라지기 시작하였던 점 등을 종합적으로 고려하면, [내용 추가 일자: 2020년 3월 15일] 동물 세포의 크기는 약 10마이크로미터, 박테리아의 크기는 약 1마이크로미터, 그리고 이 신종 코로나 바이러스의 크기는 약 0.1마이크로미터라고 하는데, 만약에 대기(大氣, atmosphere)가 일정 수준 이상 고온다습하게 되면, 인간의 몸의 동일한 크기의 단위 표면(unit surface)에 이 신종 코로나바이러스가 달라붙으려고 하는 여건/상황 아래에서, (i) 일정 수준 이상의 고온다습한 대기(大氣, atmosphere)의 영향으로 인하여, 다른 시기보다 상대적으로, 이미 엄청나게 불어난 다양한 종류의 미생물들이, 이 신종 코로나바이러스보다, 인간의 몸의 동일한 크기의 단위 표면(unit surface)에 더 많이 달라붙을 가능성이 높아질 것이기 때문에, 따라서 그 결과로서, 대기(大氣, atmosphere)가 고온다습하지 않을 시기와 비교하여, 이 신종 코로나바이러스가 인간의 몸의 동일한 크기의 단위 표면(unit surface)에 달라붙을 가능성이 상대적으로 낮아질 것이기 때문에, 그리고 여기에다, 추가적으로, (ii) 일정 수준 이상의 고온다습한 대기(大氣, atmosphere)의 영향으로 인하여, 다른 시기보다 상대적으로, 이미 엄청나게 불어난 다른 미생물들이 분비하는 다양한 종류의 분비물질들이, (A) 이 신종 코로나바이러스의 활동을 저해할 수도 있을 것이기 때문에, 그리고/혹은 (B) 이 신종 코로나바이러스의 자연적 소멸을 촉진할 수도 있을 것이기 때문에, 그러나
(iii) 바로 위의 (i)과 (ii)에서 말씀드린 자연 법칙들 아래에서 형성되는 바를, 밀폐된 실내에서 인간들이, 예를 들어, 가습기(humidifier) 등의 장치/도구들을 사용하여, 인위적으로/인공적으로 구현하는 것이 매우 힘들다고 생각하기 때문에, [이상, 2020년 3월 15일자 내용 추가 끝]
많이 부족한 죄인인, 문외한인, 필자가 생각하더라도, 예를 들어, 중국 지역과 우리나라 지역 둘 다에 고온다습한 장마철이 시작되어야 비로소 현재 창궐하여 여전히 확산 중인 우한 폐렴이 사라질 것이 아닌가... 하는 생각과 함께,
혹시라도 "이렇게" 진행될 경우에, 즉, "윤리(morality)의 범주에 속하는 사람의 의지(man's will), 욕구(appetite)/욕망(desire)/희망(hope)과 무관하게, 형이하학적(physical) 자연 법칙(natural principles)들에 따라" 진행될 경우에, 그 이전의 기간 몇 달 중에 사람들의 회합/모임이 요청되는 다양한 형태의 신앙 생활들, 교육 활동들, 사회 활동(social activities)들 등과 관련하여 발생할, 예상되는 여러 가지 현실적 어려움들에 대하여, 깊은 우려들을 하게 됩니다.
----- (*4) 게시자 주: 국내의 이러한 여건이, 방역 조치 결정권자들이 포함되는 국내의 유관 특정 집단의 자신들의 이해득실 관련 과도한 욕망(inordinate desire)에 의하여, 더욱 더 악화될 수도 있음에 대하여서는, 윤리의 범주에 속하는 바로 이 추가적 문제점을 구체적으로 지적하고 있는 위의 제1-3항을 꼭 읽도록 하라.
[내용 추가 일자: 2020년 3월 19일] (*5) 게시자 주: 다음은, 2020년 3월 17일자로, The NEW ENGLAND JOURNAL of MEDICINE 편집자에게 보내진 서신[제목: Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1]에서 발췌한 바인데, 이번 전염병을 야기한 신종 코로나바이러스 SARS-CoV-2가, 특히, 예를 들어, 병원, 요양병원, 요양원, 학교 교실, 학원 교실, 예배당/성소, 업무 및 상업용 고층 건물, 상가 건물, 실내 업무 공간, 유흥업소(디스코 클럽 포함), 실내 극징, 실내 연주회 장소, 실내 스포츠 센터, 사교 댄스 강습소, 실내 사교 모임 장소, 각종 실내 취미 모임 장소, 버스, 지하철 등에서 그러한 환경/여건이 형성될 수 있는, 이 바이러스의 단위 체적(unit volume)당 농도(density)가 높게 유지될 수 있는 환기가 잘 되지 않는 실내의 밀폐된 공간 안에서, 실외 대기의 온도 및 습도와 무관하게, 감염자로부터 에어로졸의 형태로, 중력의 작용과 거의 무관하게, [밀폐의 정도가 심할수록 대류(convection)보다는] 확산(diffusion)에 의하여 전파되어, 전염될 수 있음을 뒷받침하는 실험 데이터이다:
출처 1: https://www.nejm.org/doi/full/10.1056/NEJMc2004973 <----- 전문 필독 권고 출처 1-1: http://ch.catholic.or.kr/pundang/4/cb/nejmc2004973_appendix.pdf 출처 1-2: http://ch.catholic.or.kr/pundang/4/cb/nejmc2004973_disclosures.pdf 출처 1-3: http://ch.catholic.or.kr/pundang/4/cb/nejmc2004973.pdf [주: 출처 1에 게재된 논문의 pdf] (출처 1로부터 발췌 시작)
(이상, 발췌 끝)
바로 위에 발췌된 화면을 클릭하거나, 혹은 다음의 주소에 접속하면, 위의 실험 결과 데이터를 확대하여 더 잘 들여다볼 수 있다:
출처 2: http://ch.catholic.or.kr/pundang/4/cb/nejmc2004973_f1.jpg <----- 필히 보도록 하라
그리고 위의 실험 당시의 온도, 습도, 기간 등의 측정 조건들과 위의 실험 결과 데이터를 읽고 이해하는 데에 도움을 주는 이 실험 논문의 저자들의 설명들은 다음과 같다:
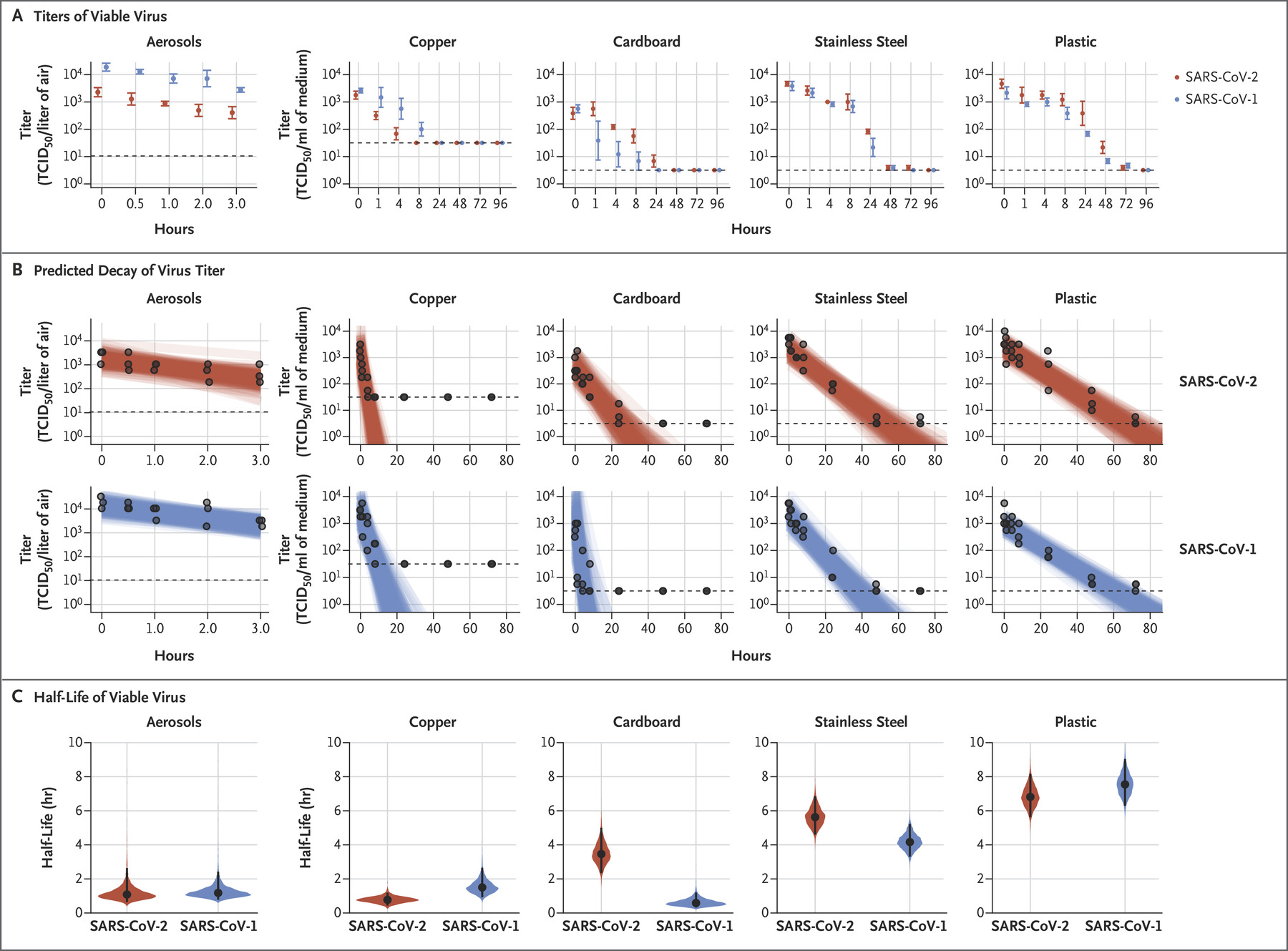
출처 1: https://www.nejm.org/doi/full/10.1056/NEJMc2004973 출처 1-1: http://ch.catholic.or.kr/pundang/4/cb/nejmc2004973_appendix.pdf (출처 1로부터 발췌 시작) SARS-CoV-2 remained viable in aerosols throughout the duration of our experiment (3 hours), with a reduction in infectious titer from 10^3.5 to 10^2.7 TCID50 per liter of air.(#1) This reduction was similar to that observed with SARS-CoV-1, from 104.3 to 103.5 TCID50 per milliliter (Figure 1A).
----- (#1) 게시자 주: (10^2.7/10^3.5)*100%를 계산하면, 약 15.85%임. 즉, 공기 중에서, 사멸되지 않고 감염시킬 수 있는 에어로졸의 총량이, 실험 시작 시점부터 3시간 후에도, 실험 시작 시점의 총량의 약 15.85%가 여전히 공기 중에 남아 있다는 결론임. ----- (이상, 발췌 끝)
(출처 1-1: Supplementary Appendix로부터 발췌 시작) 21 Virus stability in aerosols
22 Virus stability in aerosols was determined as described previously at 65% relative humidity (RH) and 23 21-23°C (Fischer et al., 2016).(#2) In short, aerosols (<5 μm) containing HCoV-19 (105.25 TCID50/mL) or 24 SARS-CoV-1 (106.75-7 TCID50/mL) were generated using a 3-jet Collison nebulizer and fed into a Goldberg 25 drum to create an aerosolized environment. Aerosols were maintained in the Goldberg drum and samples 26 were collected at 0, 30, 60, 120 and 180 minutes post-aerosolization on a 47mm gelatin filter (Sartorius). 27 Filters were dissolved in 10 mL of DMEM containing 10% FBS. Three replicate experiments were 28 performed.
----- (#2) 게시자 주: 다음의 주소들에 접속하면, 이 논문을 읽을 수 있다: 출처 1-4: https://academic.oup.com/jid/article/214/suppl_3/S290/2388091 (이상, 발췌 끝)
(바로 위 출처 1에 제시된 표를 확대하면 가지게 되는 화면의 하단으로부터 발췌 시작) Figure 1. Viability of SARS-CoV-1 and SARS-CoV-2 in Aerosols and on Various Surfaces.
As shown in Panel A, the titer of aerosolized viable virus is expressed in 50% tissue-culture infectious dose (TCID50) per liter of air. Viruses were applied to copper, cardboard, stainless steel, and plastic maintained at 21 to 23°C and 40% relative humidity over 7 days. The titer of viable virus is expressed as TCID50 per milliliter of collection medium. All samples were quantified by end-point titration on Vero E6 cells. Plots show the means and standard errors ( bars) across three replicates. As shown in Panel B, regression plots indicate the predicted decay of virus titer over time; the titer is plotted on a logarithmic scale. Points show measured titers and are slightly jittered (i.e., they show small rapid variations in the amplitude or timing of a waveform arising from fluctuations) along the time axis to avoid overplotting. Lines are random draws from the joint posterior distribution of the exponential decay rate (negative of the slope) and intercept (initial virus titer) to show the range of possible decay patterns for each experimental condition. There were 150 lines per panel, including 50 lines from each plotted replicate. As shown in Panel C, violin plots indicate posterior distribution for the half-life of viable virus based on the estimated exponential decay rates of the virus titer. The dots indicate the posterior median estimates, and the black lines indicate a 95% credible interval. Experimental conditions are ordered according to the posterior median half-life of SARS-CoV-2. The dashed lines indicate the limit of detection, which was 3.33×100.5 TCID50 per liter of air for aerosols, 100.5 TCID50 per milliliter of medium for plastic, steel, and cardboard, and 101.5 TCID50 per milliliter of medium for copper. (이상, 발췌 끝)
그리고 다음의 주소에 접속하면, "Interview with Dr. Eric Rubin and Dr. Lindsey Baden on new research on possible treatments for Covid-19"을 담은 mp3 파일을 청취할 수 있다.. 국내의 감염병 전공 의사들과 보건의학 전공 의료진들의 청취를 강력하게 권고드린다:
출처 4: http://ch.catholic.or.kr/pundang/4/cb/NEJMdo005731.mp3 [이상, 2020년 3월 19일자 내용 추가 끝]
(*6) 게시자 주: (1) 여기서 말하는 "한 개의 연(緣, condition, 조건)"이란, 정의에 의하여(by definition), 미생물들의 활발한 활동들의 필요 조건들인, 양분, 온도, 습도로 불리는, 세 개의 연(緣, conditions, 조건)들의 한 결과로서, "다른 미생물들이라는 다른 인(因, cause, 원인)들과 결합하여 이들 연(緣, conditions, 조건)들이 낳는, 더 근접한(more proximate), 한 개의 연(緣, condition, 조건)"을 말한다.
(2) 그리고 다음의 주소들에 접속하면, 여기서 사용된 용어들의 정의(definitions)들을 학습할 수 있다: http://ch.catholic.or.kr/pundang/4/soh/1554.htm <----- 필독 권고 http://ch.catholic.or.kr/pundang/4/soh/1363.htm <----- 필독 권고 ----- [이상, 2020년 2월 8일 01:50 내용 추가 끝]
[내용 추가 일자: 2020년 2월 6일 17:56] 3. 다음에 발췌된 바는, 중국 후베이성 우한 시 수산시장에서 신종 코로나바이러스에 감염된 자들을 치료한, 우한 South Central Hospital ICU(Intensive Care Unit, 중환자실/집중치료실) 소속의 의사와 인터뷰한 내용입니다. 도대체 중국 후베이성 우한 시에서 이 전염병의 창궐 초기에 우한 소재 한 병원의 의료진과 중국 정부의 대음에 있어 실제로 무슨 일들이 벌어졌는지에 대하여, 국내의 의료진들을 포함하여, 궁금증을 가진 분들이 많을 것으로 생각되어, 여기에 발췌하였습니다:
출처: http://ch.catholic.or.kr/pundang/4/Wuhan/Life_and_Death_in_a_Wuhan_Coronavirus_ICU.htm (발췌 시작) Feb 06, 2020 07:40 AM Reporter’s Notebook: Life and Death in a Wuhan Coronavirus ICU[차이신(CaiXin)] 기자 수첩: 우한 코로나바이러스 중환자실/집중치료실(ICU) 안에서 삶과 죽음
By Xiao Hui
(Wuhan)--In the coronavirus epidemic, doctors on the front lines take on the greatest risk and best understand the situation. Peng Zhiyong, director of acute medicine at the Wuhan University South Central Hospital, is one of those doctors. (우한) -- 이 코로나바이러스 전염병에 있어, 방어선들에 있는 의사들이 가장 커다란 위험을 떠맡고 있으며 그리고 그 상황을 가장 잘 이해하고 있습니다. 우한 대학교 South Central Hospital 소재 급성 내과(acute medicine)의 장(director)인, Peng Zhiyong은 바로 이러한 의사들 중의 한 명입니다. In an interview Tuesday with Caixin, Peng described his personal experiences in first encountering the disease in early January and quickly grasping its virulent potential and the need for stringent quarantine measures. 차이신(Caixin, 财新传媒)과 화요일에 있었던 한 인터뷰에서, [의사] Peng은, 1월 초에 이 질병과 처음 마주침 그리고 이 질병의 전염성이 강한 잠재력을 즉시 알아차림 그리고 엄중한 격리 조치들의 필요에 관한(in), 자신의 개인적 경험들을 설명하였습니다. As the contagion spread and flooded his ICU, the doctor observed that three weeks seemed to determine the difference between life and death. Patients with stronger immune systems would start to recover in a couple of weeks, but in the second week some cases would take a turn for the worse. 이 접촉 전염병이 퍼져 자신의 ICU(중환자실/집중치료실)를 범람시켜감에 따라, 이 의사는 3주(3 weeks)가 삶과 죽음 사이의 차이를 결정하는 것 같음을 관찰하였습니다. 더 강한 면역 체계들을 가진 환자들은 2-3주 안에 회복하기 시작할 것이나, 그러나 두 번째 주 중에 어떤 사례(cases)들은 악화되는 쪽으로 돌아설 것입니다. In the third week, keeping some of these acute patients alive might require extraordinary intervention. For this group, the death rate seems to be 4% -5%, Peng said. After working his 12-hour daytime shifts, the doctor spends his evenings researching the disease and has summarized his observations in a thesis. 세 번째 주 중에, 바로 이들 급성의 환자들 중의 일부를 살아있게 하는 것은 특별한 개입(extraordinary intervention)을 요구할 것입니다. 바로 이 집단의 경우에, 치사율(death rate)은 4%-5%인 것 같다고 Peng은 말하였습니다. 자신의 12시간 주간 교대제 일을 마친 후에, 이 의사는 자신의 밤들을 이 질병에 대하여 연구하는 데에 보내며 그리고 자신이 관찰한 바를 한 편의 논문에 요약하였습니다. The doctors and nurses at his hospital are overwhelmed with patients. Once they don protective hazmat suits, they go without food, drink and bathroom breaks for their entire shifts. That’s because there’s aren’t enough of the suits for a mid-shift change, he said. 그의 병원에서 일하는 의사들과 간호사들은 환자들에 압도당하였습니다. 일단 그들이 위험 물질에 안전 장치를 제공하는(protective) 옷들을 입으면, 그들은 음식, 음료 그리고 화장실 휴식들 없이 자신들의 전체 교대제를 위하여 나아갑니다. 바로 이것은 한 번의 중간 교체를 위한 옷들이 충분하지 않기 때문이라고, 그가 말하였습니다. Over the past month on the front lines of the coronavirus battle, Peng has been brought to tears many times when forced to turn away patients for lack of staffing and beds. He said what really got to him, though, was the death of an acutely ill pregnant woman when treatment stopped for lack of money ― the day before the government decided to pick up the costs of all coronavirus treatments. 이 코로나바이러스 전쟁의 방어선들에서 지난 한 달에 걸쳐, Peng은 의료진과 병상들의 부족 때문에 롼자들을 외면하도록 강제되었을 때에 수없이 눈물을 흘리게 되었습니다. 그는 다음과 같이 말하였습니다: 그럼에도 불구하고, 그에게 정말로 영향을 준(got to) 바는, [중국] 정부가 모든 코로나바이러스 치료들의 비용의 지불을 떠맡겠다고 결정하기 하루 전에, 돈의 부족 때문에 치료를 중단하였을 때에 한 명의 급성의 병든 임신 중인 여인의 죽음이었습니다. Here’s our interview with the ICU doctor: 다음은 이 ICU(중환자실/집중치료실) 의사와 가진 우리의 인터뷰 입니다: 게시자 주: 누구나 알아야 한 필요가 있다고 생각되는 아래의 본문 중의 특정 단락들에는 필자가 마련한 우리말 번역문들을 추가하였습니다. Screening criteria were too tough in the beginning 처음에, 걸러내는 기준들이 너무 엄격하였습니다 Caixin: When did you encounter your first novel coronavirus patient? Caixin: 언제 첫 번째 신종 코로나바이러스 환자와 마주쳤는지요? Peng Zhiyong: Jan. 6, 2020. There was a patient from Huanggang who had been refused by multiple hospitals, who was sent to the South Central Hospital emergency room. I attended the consultation. At the time, the patient’s illness was already severe, and he had difficulty breathing. I knew right then that he contracted this disease. We debated at length whether to accept the patient. If we didn’t, he had nowhere to go; if we did, there was a high likelihood the disease would infect others. We had to do a very stringent quarantine. We decided to take the patient in the end. Pen Zhiyong: 2020년 1월 6일. 다수의 병원들에 의하여 거부되어 온 황강(Huanggang, 후베이성 동부에 위치한 지급시) 출신의 환자가 한 명 있었는데, 그가 South Central Hospital 응급실로 보내졌습니다. 저는 전문가 협의회(consultation)에 참석하였습니다. 바로 그 시점에, 이 환자의 병은 이미 심각하였으며, 그리하여 그는 숨을 쉬는 데에 어려움을 가지고 있었습니다. 저는 그 즉시 그가 바로 이 질병에 감염되었음을 알았습니다. 우리는 장시간에 걸쳐 이 환자들 받아들일 것인지에 대하여 토론하였습니다. 만약에 우리가 그러지 않으면, 그는 갈 곳이 없었으며, 그리고 만약에 우리가 그를 받아들이면, 이 질병이 다른 이들을 감염시킬 높은 가능성이 있었습니다. 우리가 매우 엄중한 격리를 하여야 하기 때문이었습니다. 우리는 마침내 그를 받아들이기로 결정하였습니다. I called the hospital director and told him the story, including the fact that we had to clear the hospital room of other patients and to remodel it after SARS standards by setting up a “contamination area,” “buffer area,” “cleaning area,” and separate the living areas of the hospital staff from the patients’. 저는 병원장에게 전화하였으며 그리고 우리가 다른 환자들의 병원 공간(hospital room)을 치워야 하고 그리고, 사스(SARS) 기준들에 따라서(after) 한 개의 "오염 지역", "완충 지역", "청결 지역"을 설정함으로써, 이 공간을 개조하여야 한다는 사실을 포함하여, 이 환자에 대한 이야기를 그에게 말하였습니다. On Jan. 6, with the patient in the emergency room, we did quarantine remodeling in the emergency room and did major renovations to the ICU (intensive care unit). South Central Hospital’s ICU has 66 beds in total. We kept a space dedicated to coronavirus patients. I knew the infectiousness of the disease. There were bound to be more people coming in, so we set aside 16 beds. We did quarantine renovations on the infectious diseases area because respiratory illnesses are transmitted through the air, so even air has to be quarantined so that inside the rooms the air can’t escape. At the time, some said that the ICU had a limited number of beds and 16 was excessive. I said it wasn’t excessive at all. 1월 6일 바로 그날, 이 환자가 응급실에 있는 상태에서, 응급실 안에서 격리 개조(quarantine remodeling)를 행하였으며 그리고 ICU(중환자실/집중치료실)에 대한 주된 개조들을 행하였습니다. South Central Hospital의 중환자실/집중치료실(ICU)은 총 66개의 병상(病床)들을 가지고 있습니다. 우리는 코로나바이러스 환자들에게 할애된 한 공간(a space)을 계속 유지하게 하였습니다. 저는 이 질병의 전염력을 알고 있었습니다. 더 많은 사람들이 필연적으로 들어 오게 될 것이기에(be bound to), 그래서 우리는 16 병상들을 확보하였습니다. 왜냐하면 호흡기 질환들은 공기를 통하여 전염되기 때문에 우리는 이 전염성 질병에 대하여 격리 개조들(quarantine renovations)을 정말로 하였는데, 따라서 실내 안에 있는 공기가 빠져나갈 수 없도록 하고자 심지어 공기마저도 격리되어야 하였습니다 [주: 음압이 유지되는 격리 병실을 마련하였음을 말하고 있는 듯 함]. 바로 그 시점에, 어떤 이들은 이 중환자실/집중치료실(ICU)은 제한된 숫자의 병상들을 가지고 있고 그리하여 16 병상들은 과도하다고 말하였습니다. [그러나] 저는 그것이 결코 과도하지 않다고 말해주었습니다. Caixin: You predicted back in January that there would be person-to-person transmission and even took quarantine measures. Did you report the situation to higher-ups? Caixin: 당신은 거슬어 올라가 1월달에 인간-대-인간 전염(person-to-person transmission)이 있을 것이며 그리하여 심지어 격리 조치들을 취하여야 한다고 예측하였습니다. 당신은 이 상황을 [병원장보다] 더 높은 분(higher-ups)들에게 보고하였는지요? Peng: This disease really did spread very fast. By Jan. 10, the 16 beds in our ICU were full. We saw how dire the situation was and told the hospital’s leadership that they had to report even higher. Our head felt it was urgent too and reported this to the Wuhan city health committee. On Jan. 12, the department sent a team of three specialists to South Central to investigate. The specialists said that clinical symptoms really resembled SARS, but they were still talking about diagnosis criteria, that kind of stuff. We replied that those standards were too stringent. Very few people would get diagnosed based on those criteria. The head of our hospital told them this multiple times during this period. I know other hospitals were doing the same. Peng: 이 질병은 매우 빠르게 실제로 퍼졌습니다. 1월 10일자로, 우리의 중환자실/집중치료실(ICU)의 16 병상들은 가득 찼습니다. 우리는 이 상황이 얼마나 급박한지 보았으며 그리하여 우리 병원의 수뇌부(leadership)에게 그들이 심지어 더 높은 분들께 보고하여야 함을 말해주었습니다. 우리의 우두머리(head)도 또한 상황이 급박하다고 느꼈으며 그리고 이것을 우한 시(Wuhan City) 보건 위원회(health committee)에 보고하였습니다. 1월 12일에, 이 과[the department, 즉, 이 보건 위훤회]는 [이것을] 조사하기 위하여 세 명의 전문가들로 구성된 한 개의 팀을 South Central [Hospital]로 파견하였습니다. 이 전문가들은 임상 증상들은 실제로 사스(SARS)와 유사하나, 그러나 그들은 검진 기준(diagnosis criteria)들 등과 같은 것들에 관하여 여전히 계속 말하였습니다. 우리는 바로 그러한 기준들은 너무 엄격하다고 답변하였습니다. 바로 그 기준들에 근거하면 매우 적은 사람들이 검진을 받게 될 것이기 때문이었습니다. 우리 병원의 우두머리도 또한, 바로 이 기간 동안에, 그들에게 바로 이 점을 여러 번에 걸쳐 말하였습니다. 저는 다른 병원들도 동일한 말을 하고 있음을 알고 있었습니다. Before this, the specialists already went to Jinyintan Hospital to investigate and made a set of diagnosis criteria. You had to have had exposure to the South China Seafood Market, you needed to have had a fever and test positive for the virus. You had to meet all three criteria in order to be diagnosed. The third one was especially stringent. In reality, very few people were able to test for a virus. 바로 이 방문 전에, 이 전문가들은 이미, 조사하기 위하여 Jinyintan Hospital 에 갔으며 그리고, 다음과 같은, 검진 기준들의 한 조를 마련하였습니다: (i) 그대는 South China 수산시장 쪽으로 노출되었어야 하고, (ii) 그대는 반드시 어떤 발열(a fever)을 가져야하며 그리고 (iii) 반드시 이 바이러스에 대하여 양성 반응을 보여야(test positive) 한다. On Jan. 18, the high-level specialists from the National Health Commission came to Wuhan, to South Central Hospital to inspect. I told them again that the criteria were too high. This way it was easy to miss infections. I told them this was infectious; if you made the criteria too high and let patients go, you’re putting society in danger. After the second national team of specialists came, the criteria were changed. The number of diagnosed patients rose quickly. 1월 18일에, 국가 보건 위원회로부터 고위급 전문가들이 조사하가 위하여 우한 시 쪽으로, South Central Hospital 쪽으로 왔습니다. 저는 그들에게 또다시 이 기준들이 너무 높다고 말하였습니다. 바로 이러한 방식으로는, 감염(infections)들을 놓치는 것이 십상이기 때문이었습니다. 이 질병이 전염성이 있으며(infectious), 만약에 여러분들이 너무 높은 기준들을 마련하여 그리하여 환자들로하여금 돌아가게 하면, 여러분들이 사회릉 위험에 처하게 하는 것이라고 제가 그들에게 말하였습니다. 전문가들로 구성된 두 번째 국가 팀이 온 이후에, 이 기준들이 바뀌어졌습니다. [그 이후로] 검진/진단을 받게 되는 환자(diagnosed patients)들의 숫자는 빠르게 증가하였습니다.
Caixin: What made you believe that the new coronavirus could be transmitted between people? Caixin: 당신으로 하여금 이 신종 코로나바이러스가 사람들 사이에서 전염될 수 있음을 믿게 한 것이 무엇이었는지요? Peng: Based on my clinical experience and knowledge, I believed that the disease would be an acutely infectious disease and that we had to do high-level protection. The virus isn’t going to change based on man’s will. I felt we needed to respect it and act according to science. Under my requirements, South Central Hospital’s ICU took strict quarantine measures, and as a result, our department only had two infections. As of Jan. 28, of the entire hospital’s medical personnel, only 40 have been infected. This is way less compared with other hospitals in terms of percentage of total medical staff. Peng: 저의 임상 경험과 지식에 근거하면, 이 질병이 하나의 급성으로 전염성이 강한 질병일 것임을 그리하여 우리가 높은 수준의 안전 장치(protection)를 하여야 함을, 저는 믿었습니다. 이 바이러스는 사람의 의지[man's will, 사람의 이성적 욕구(rational appetite)]에 근거하여 변화하지 않을 것입니다. 우리가 이 점을 고려에 넣고 그리고 과학에 따라 행동할 필요가 있음을, 저는 느꼈습니다. 저의 요구들 아래에서, South Central Hospital의 ICU(중환자실/집중치료실)는 엄격한 격리 조치들을 취하였으며, 그리하여 그 결과, 우리의 과(department)는 오로지 두 건의 감염(infections)들만을 가졌습니다. 1월 29일자로, 이 병원 전체의 의료 인원들 중에서, 오로지 40명만이 감염되었습니다. 이것은 전체 의료진의 퍼센트로 환산하여(in terms of) 다른 병원들과 비교하였을 때에 훨씬 더 적은(way less) 것입니다. It pains us to see the coronavirus develop to such a desperate state. But the priority now is to treat people; do everything we can to save people. Fatality rate for acute patients is 4%-5%; 3 weeks determine life and death 급성의 환자들의 경우에 치사율이 4%-5%이며, 그리고 3주(3 weeks)가 삶과 죽음을 결정합니다 Caixin: Based on your clinical experience, what’s the disease progression of the new coronavirus? Caixin: 당신의 임상 경험에 근거하면, 이 신종 코로나바이러스의 질병 진행(disease progression)은 어느 정도인지요? Peng: Lately I’ve been spending the daytime seeing patients in the ICU, then doing some research in the evenings. I just wrote a thesis. I drew on data from 138 cases that South Central Hospital had from Jan. 7-28 and attempted to summarize some patterns of the novel coronavirus. Peng: 최근에 저는 ICU(중환자실/집중치료실)에서 환자들을 보면서 낮시간을 보내 왔으며, 그러고나서 밤들에 일부 연구를 하였습니다. 저는 한 편의 논문을 방금 썼습니다. 저는 South Central Hospital이 1월 7-29일 동안 가졌던 138건의 사례들로부터 데이터를 뽑아내었으며 그리고 이 신종 코로나바이러스의 어떠한 패턴들을 요약하고자 시도하였습니다. A lot of viruses will die off on their own after a certain amount of time. We call these self-limited diseases. I’ve observed that the breakout period of the novel coronavirus tends to be three weeks, from the onset of symptoms to developing difficulties breathing. Basically going from mild to severe symptoms takes about a week. There are all sorts of mild symptoms: feebleness, shortness of breath, some people have fevers, some don’t. Based on studies of our 138 cases, the most common symptoms in the first stage are fever (98.6% of cases), feebleness (69.6%), cough (59.4%), muscle pains (34.8%), difficulties breathing (31.2%), while less common symptoms include headaches, dizziness, stomach pain, diarrhea, nausea, vomiting. 바이러스들의 많은 종류들은 시간의 일정한 양 이후에 스스로 죽어 사라질 것입니다. 우리는 이것들을 스스로-한정된 질병(self-limited diseases)들이라고 부릅니다. 이 신종 코로나바이러스의 발병 기간은, 증상들의 시작부터 호흡 곤란들로 발전하기까지, 3주들인 경향이 있음을 관찰하였습니다. 기본적으로 가벼운 증상들로부터 심한 증상들까지 가는 데에 약 한 주일이 걸립니다. 다음과 같은 가벼운 증상들의 모든 종류들이 있습니다: 힘이 없음(feebleness), 숨이 참(shortness of breathing), 일부 사람들은 발열(fevers)들을 가지나, 일부는 그렇지 않습니다. 우리의 138 사례들에 대한 학습(studies)들에 근거하면, 첫 번째 단계에 있어 가장 공통인 증상(the most common symptoms)들은 발열(fever)(98.6%), 힘이 없음(feebleness)(69.6%), 기침(cough)(59.4%), 근육통(muscle pains)들(34.8%), 숨이 참(difficulties breathing)(31.2%)이며, 이와는 달리 덜 공통인 증상(less common symptoms)들은 두통(headaches)들, 어지러움(dizziness), 위장 통증(stomach pain), 설사(diarrhea), 메스꺼움(nausea), 구토 행위(vomitting)를 포함합니다. But some patients who enter the second week will suddenly get worse. At this stage, people should go to the hospital. Elderly with underlying conditions may develop complications; some may need machine-assisted respiration. When the body’s other organs start to fail, that’s when it becomes severe, while those with strong immune systems see their symptoms decrease in severity at this stage and gradually recover. So the second week is what determines whether the illness becomes critical. 그러나 두 번째 주에 들어가는 일부 환자들은 갑자기 악화될 것입니다. 바로 이 단계에서, 사람들은 병원에 반드시 가야 합니다. 기저 질환들을 가진 노인들은 합병증들을 일으킬 수도 있으며, 그리하여 어떤 이들은 기계가 보조하는 호흡이 필요할 수도 있습니다. 신체의 다른 장기/기관(organs)들이 작동하지 않기 시작하면, 바로 이 시점이 그것이 심각하게 될 때이며, 이와는 달리 강한 면역 체계들을 가진 자들은 바로 이 단계에서 고통에 있어 그들의 증상들이 줄어듬을 보며 그리고 점차적으로 회복합니다. 따라서 이 두 번째 주(the second week)가 이 병이 위독하게(critical) 되느냐를 결정하는 바로 그 기간입니다. The third week determines whether critical illness leads to death. Some in critical condition who receive treatment can raise their lymphocyte, a type of white blood cell, and see an improvement in their immune systems, and have been brought back, so to speak. But those whose lymphocyte numbers continue to decline, those whose immune systems are destroyed in the end, experience multiple organ failure and die. 세 번째 주는 위독한 병이 죽음에 이르게 할 것인지를 결정합니다. 치료를 받는, 위독한 상태에 있는, 일부 환자들은, 백혈구의 한 형식인, 자신들의 림프구(lymphocyte)를 북돋울(raise) 수 있으며, 그리하여 그들의 면역 체계들에 있어 어떤 개선을 보며, 그리하여, 말하자면, 되돌려지게 되게 될 것입니다. 그러나 림프구 숫자들이 계속하여 줄어드는 바로 그들은, 면역 체계들이 결국에 파괴되는 바로 그들이며, 복합장기부전(複合臟器不全)(multiple organ failure, MOF)를 경험하고 그리하여 죽습니다. For most, the illness is over in two weeks, whereas for those for whom the illness becomes severe, if they can survive three weeks they’re good. Those that can’t will die in three weeks. 대부분의 경우에, 이 병은 2주 안에 끝나나, 이와는 달리 이 병이 심각하게 되는 자들은, 만약에 그들이 3주를 생존할 수 있으면 그들은 다행입니다(good). 그럴 수 없는 자들은 3주 안에 장차 죽을 것입니다.
Caixin: Will you please give more details on clinical research? What percentage of cases would develop from mild conditions to severe conditions? What percentage of serious cases would develop into life-threatening cases? What is the mortality rate? Caixin: 임상 연구에 대한 더 자세한 내용들을 제공해 주시겠는지요? 사례들의 몇 퍼센트가 가벼운 상태들로부터 위중한 상태들로 발전할 것인지요? 심각한 사례들의 몇 퍼센트가 생명이 위험한 사례들로 발전할 것인지요? 치사율은 어느 정도인지요? Peng: Based on my clinical observations, this disease is highly contagious, but the mortality rate is low. Those that progressed into the life-threatening stage often occurred in the elderly already with chronic diseases. Peng: 저의 임상 관찰(clinical observations)들에 근거하면, 이 질병은 전염성이 높으나, 그러나 치사율은 [사스 혹은 메르스보다] 낮습니다. 생명이 위험한 단계로 진행한 자들은 만성 질병들을 이미 가지고 있는 노인들에서 자주 발생하였습니다. As of Jan. 28, of 138 cases, 36 were in the ICU, 28 recovered, five died. That is to say, the mortality rate of patients with severe conditions was 3.6%. Yesterday (Feb. 3), another patient died, bringing the mortality rate to 4.3%. Given patients in the ICU, it is likely to have more deaths. The mortality rate is also likely to edge up but not significantly. 1월 28일자로, 138 사례들 중에서 36 사례들이 ICU(중환자실/집중치료실)에서였으며, 28 사례들은 회복되었고, 다섯 사례들은 죽었습니다. 다시 말해서, 심각한 상태들을 가진 환자들의 치사율은 3.6% (즉, 5/138 x 100 = 3.6%)였습니다. 어제(2월 3일), 또다른 환자가 죽었기에, 이 치사율을 4.3%로 끌어 올렸습니다. ICU(중환자실/집중치료실)에 있는 환자들의 경우에, 더 많은 죽음들을 가질 가능성이 있습니다. 치사율은 올라갈 가능성이 있으나 그러나 괄목할만 하지는 않을 것입니다. Those hospitalized tend to have severe or life-threatening conditions. Patients with slight symptoms are placed in quarantine at home. We have not gathered data on the percentage of cases that progress from slight symptoms to serious symptoms. If a patient goes from serious conditions to life-threatening conditions, the patient will be sent to the ICU. Among 138 patients, 36 were transferred to the ICU, representing 26% of all patients. The percentage of deaths among life-threatening cases is about 15%. The mean period to go from slight conditions to life-threatening conditions is about 10 days. Twenty-eight patients recovered and were discharged. Right now, the recovery rate is 20.3% while other patients remain hospitalized. 바로 이들 [병원에] 입원한 자들은 심각하거나 혹은 생명이 위험한 상태들을 가지는 쪽으로 기울어지는 경향이 있습니다. 경미한 증상들을 가진 환자들은 집에서 격리 상태에 놓여집니다. 경미한 증상들로부터 심각한 증상들로 진행한 사례들의 퍼센트에 대한 데이터를 우리는 취합하지 않아 왔습니다. 만약에 한 환자가 심각한 상태로부터 생명이 위험한 상태들로 가면, 이 환자는 ICU(Intensive Care Unit, 중환자실/집중치료실)로 보내질 것입니다. 138명의 환자들 가운데에서, 36명이 ICU로 이송되었는데, [이들은] 모든 환자들의 26%를 나타냅니다. 생명이 위험한 환자들 가운데에서 죽음들의 퍼센트는 약 15%입니다. 경미한 상태들로부터 생명이 위험한 상태들로 가는 평균 기간은 약 10일입니다. 28명의 환자들은 회복하였으며 그리하여 퇴원하게 되었습니다. 바로 지금, 회복률은 20.3%이며, 이와는 달리 다른 환자들은 입원한 상태로 남아 있습니다. It is notable that 12 cases were linked to South China Seafood Market; 57 were infected while being hospitalized, including 17 patients already hospitalized in other departments; and 40 medical staff, among 138 cases (as of Jan. 28). That demonstrates that a hospital is a high-risk zone and appropriate protection must be taken. 138 사례들 중에서, 12 사례들이 [우한의] 남중국 수산 시장(South China Seafood Market) 쪽으로 연결이 되었고, 그리고 57 사례들은, 다른 과(department)들에 이미 입원한 17명의 환자들을 포함하여, 입원하고 있는 동안에 감염되었으며, 그리고 40 사례들은 의료진이었음은 주목할 만 합니다. 바로 이것은 병원이 하나의 위험성이 큰 영역(zone)이며 그리고 적절한 보호/방위(protection)가 취하여져야 함을 입증합니다. Caixin: What is the highest risk a serious patient faces? Caixin: 한 명의 심각한 환자가 직면할 가장 높은 위험은 무엇인지요? Peng: The biggest assault the virus launches is on a patient’s immune system. It causes a fall in the count of lymphocytes, the damage in the lungs and shortness of breath. Many serious patients died of choking. Others died of the failure of multiple organs following complications in their organs resulting from a collapse of the immune system. Peng: 이 바이러스가 가하는 가장 커다란 공격은 환자의 면역 체계에 대하여서 입니다. 이 공격은 림프구(lymphocytes)들의 개수(個數)에 있어 떨어짐을, 허파들에 손상을 그리하여 숨이 참(shortness of breath)을, 야기합니다. 다수의 심각한 환자들은 숨막힘(choking) 때문에 죽었습니다. 다른 이들은, 면역 체계의 붕괴로부터 유래하는 그들의 장기/기관(organs)들에 있는 합병증들에 뒤따르는, 다중 장기들의 기능 부전(不全)(failure) [MOF] 때문에 죽었습니다. Caixin: A 39-year-old patient in Hong Kong suffered from cardiac arrest, and his death ensued quickly. A few patients did not have severe symptoms upon the onslaught of the virus or in early stages, but they died suddenly. Some experts argue that the virus triggers a cytokine storm, which ravages the stronger immune system of young adults. Eventually excessive inflammations caused by cytokine result in the higher mortality rate. Have you seen such a phenomenon in the coronavirus outbreak? Caixin: 홍콩에서 한 명의 환자가 심장 마비로 고통을 받았으며, 그리고 그의 죽음이 급하게 뒤따랐습니다. 몇 명의 환자들은, 이 바리러스의 맹공격을 받자마자 혹은 초기의 단계들에서, 심각한 증상들을 가지지 않았으나, 그러나 그들은 갑자기 죽었습니다. 일부 전문가들은 이 바이러스가, 젊은이(young adults)들의 더 강한 면역 체계를 파괴하는(ravages), 시토킨 폭풍/사이토카인 폭풍(a cytokine storm)을 촉발시킨다고 주장합니다. 결국에 시토킨 폭풍/사이토카인 폭풍에 의하여 야기되는 과도한 염증들이 더 높은 치사율을 초래합니다. 당신은 이 코로나바이러스 발발에서 그러한 현상을 보았는지요? Peng: Based on my observations, a third of patients exhibited inflammation in their whole body. It was not necessarily limited to young adults. The mechanism of a cytokine storm is about whole-body inflammation, which leads to a failure of multiple organs and quickly evolves into the terminal stage. In some fast-progressing cases, it took two to three days to progress from whole-body inflammation to the life-threatening stage. Peng: 저의 관찰들에 근거하면, 환자들의 1/3이 그들의 전체 몸에서 염증을 드러내었습니다. 이것은 젊은이들에게만 반드시(not necessarily) 제한되지 않았습니다. 시토킨 폭풍/사이토카인 폭풍의 메카니즘은 전체 몸의 염증에 관한 것이며, 이 염증이 다중 장기들의 기능 부전(不全)(failure)[MOF]에 이르게 하고 그리하여 말기의 단계 쪽으로 급하게 진전합니다. 일부 빠르게 진행하는 사례들에 있어, 전체 몸의 염증으로부터 생명이 위험한 단계로 진행하는 데에 2일에서 3일이 걸렸습니다. Caixin: How do you treat serious and life-threatening cases? Peng: For serious and life-threatening cases, our main approach is to provide oxygen, high-volume oxygen. At first noninvasive machine-pumped oxygen, followed by intubated oxygen if conditions worsen. For life-threatening cases, we use ECMO (extracorporeal membrane oxygenation, or pumping the patient’s blood through an artificial lung machine). In four cases, we applied ECMO to rescue patients from the verge of death. Currently there are no special drugs for the coronavirus. The primary purpose of the ICU is to help patients sustain the functions of their body. Different patients have different symptoms. In case of shortness of breath, we provided oxygen; in case of a kidney failure, we gave dialysis; in case of a coma, we deployed ECMO. We provide support wherever a patient needs it to sustain their life. Once the count of lymphocytes goes up and the immune system improves, the virus will be cleared. However, if the count of lymphocytes continues to fall, it is dangerous because the virus continues to replicate. Once a patient’s immune system is demolished, it is hard to save a patient. Caixin: There is news of some drugs that work. People are hopeful of the effect of U.S.-made remdesivir, which cured the first case in the United States. What do you think of the drugs? Peng: There are not 2019 novel coronavirus-targeted drugs so far. Some patients may recover after taking some drugs along with supportive treatment. But such individual cases do not indicate the universal effect of the drugs. The effect is also related to how serious each case is and their individual health conditions. People want a cure urgently, and that is understandable. But we need to be cautious. Caixin: Do you have any advice for coronavirus-infected patients? Peng: The most effective approach to the virus epidemic is to control the source of the virus, stem the spread of the virus and prevent human-to-human transmission. My advice for a patient is going to a special ward for infectious diseases, early detection, early diagnosis, early quarantine and early treatment. Once it has developed into a severe case, hospitalization is a must. It is better to contain the disease at an early stage. Once it reaches the life-threatening stage, it is way more difficult to treat it and requires more medical resources. With regard to life-threatening cases, try to save them with ICU measures to reduce the mortality rate. Sad story of a pregnant patient Caixin: How many patients with life-threatening conditions have you treated? How many have recovered? Peng: As of Feb. 4, six patients in the ICU of South Central Hospital died. Eighty percent of them have been improving, a quarter are approaching their discharge and the remainder are still recovering in segregated wards. The patient who impressed me most came from Huanggang. He was the first to be saved with the assistance of ECMO. He had contact with South China Seafood Market and was in very serious conditions. He was transferred to the ICU and we saved him with ECMO. He was discharged from the hospital Jan. 28. Caixin: What are your work load and pace like? Peng: The work in the ICU is overloaded. There are three patient wards with 66 beds in South Central Hospital, housing 150 patients. Since Jan. 7 when we received the first patient, no one took any leave. We took turns to work in the ICU. Even pregnant medical staff did not take leave. After the epidemic got worse, none of the medical staff ever went home. We rest in a hotel near the hospital or in the hospital. In the segregated ward, we wear level-3 protective gear. One shift is 12 hours for a doctor and eight hours for a nurse. Since protective gear is in a shortage, there is only one set for a medical staff member a day. We refrain from eating or drinking during our shift because the gear is no longer protective once we go to the washroom. The gear is thick, airtight and tough on our body. It felt uncomfortable at the beginning, but we are used to it now. Caixin: Did you experience a very dangerous moment? For example, in case of intubation, what do you do to prevent yourselves from being infected? Peng: It is a new coronavirus. We are not sure of its nature and its path of spread. It is not true if we say we are not afraid. Medical staff members do fear to some extent. But patients need us. When a patient is out of breath and noninvasive oxygen provision fails, we must apply intubation. The procedure is dangerous as the patient may vomit or spit. Medical staff are likely to be exposed to the danger of infection. We strictly require doctors and nurses to apply the highest-level protection. The biggest problem we face now is the shortage of protective gear. The protective stock for ICU staff is running low, although the hospital prioritizes the supply to us.
Caixin: Is there anything that moved you in particular? Did you cry? Peng: I often cried because so many patients could not be admitted to the hospital. They wailed in front of the hospital. Some patients even knelt down to beg me to accept him into the hospital. But there was nothing I could do since all beds were occupied. I shed tears while I turned them down. I ran out of tears now. I have no other thoughts but to try my best to save more lives. The most regretful thing to me was a pregnant woman from Huanggang. She was in very serious condition. Nearly 200,000 yuan (about $28,700) were spent after more than a week in the ICU. She was from the countryside, and the money for hospitalization was borrowed from her relatives and friends. Her condition was improving after the use of ECMO, and she was likely to survive. But her husband decided to give up. He cried for his decision. I wept too because I felt there was hope for her to be saved. The woman died after we gave up. And exactly the next day, the government announced a new policy that offers free treatment for all coronavirus-infected patients. I feel so sorry for that pregnant woman. The deputy director of our department told me one thing, and he cried too. Wuhan 7th Hospital is in a partnership with our hospital, South Central Hospital. The deputy director went there to help in their ICU. He found that two-thirds of the medical staff in the ICU were already infected. Doctors there were running “naked” as they knew they were set to be infected given the shortage of protective gear. They still worked there nonetheless. That was why ICU medical staff were almost all sickened. It is too tough for our doctors and nurses. Translated By Sun Huixia and Dave Yin Contact editor Bob Simison (bobsimison@caixin.com) (이상, 발췌 끝) [이상, 2020년 2월 6일 17:58 내용 추가 및 일부 문장들의 우리말 번역 끝]
[내용 추가 일자: 2020년 3월 30일] 게시자 주: 다음의 주소들에 접속하면, 본글에 이어지는 졸글들을 읽을 수 있습니다. 되도록 많은 분들이 읽으실 것을 강력하게 권고드립니다:
http://ch.catholic.or.kr/pundang/4/soh/2032.htm <----- 필독 권고 [제목: 방심과 공포 사이에는 어떤 것들이 있을까요? 형이하학적 악(physical evils)들의 종류들; 게시일자: 2020-02-22]
http://ch.catholic.or.kr/pundang/4/soh/2033.htm <----- 필독 권고 [제목: 오늘은 재의 수요일(Ash Wednesday); 게시일자: 2020-02-26]
[제목: 세속적 과도한 욕망들을 판단의 기준들로 습관적으로 계속 사용하여 형이하학적 악들의 다양한 형태들을 인위적으로 만들어 내는 자들은 인과응보/상선벌악 를 모르는 자들이다; 게시일자: 2020-03-11]
http://ch.catholic.or.kr/pundang/4/soh/2037.htm <----- 필독 권고 [제목: 신종 코로나바이러스 전염병 치료에 한약 청폐배독탕 이 도움이 된다고 합니다; 게시일자: 2020-03-17] [이상, 2020년 3월 30일자 내용 추가 끝]
---------- 작성자: 교수 소순태 마태오 (Ph.D.)
0 1,218 2
|